 Skip to content
Skip to content 
Imagine you see someone with a swollen, sore knee and a fever. Septic arthritis can hurt the joint very quickly. Studies show cartilage can get damaged in just a few hours.
It is important to find and treat it early according to the septic arthritis treatment guidelines. This helps keep the joint and the person safe.
New treatment rules for 2025 say to drain the joint fast and give antibiotics. Septic arthritis happens all over the world:
- In Thailand, about 41 out of 100,000 people have it.
- In Aboriginal Australians, 29.1 out of 100,000 get it each year.
- In New Zealand, 21 out of 100,000 get it each year.
Key Takeaways
- Act fast if you think it is septic arthritis. Early finding and treatment can stop bad joint damage.
- Drain the infected joint quickly. This takes out bacteria and lowers pressure. It keeps the joint safe.
- Give antibiotics right after you test joint fluid. This helps treatment work well and helps the patient get better faster.
- Check the patient’s progress often. Look for pain, swelling, or fever that does not get better. These signs may mean the treatment is not working.
- Help the patient move early and start rehab. This brings back joint movement and stops stiffness when the infection is gone.
Septic Arthritis Treatment Guidelines 2025
Key Recommendations
You must act fast if you think someone has septic arthritis. The 2025 guidelines say to diagnose quickly, drain the joint early, and use the right antibiotics. These steps help keep the joint safe and stop future problems.
Doctors find septic arthritis in native joints by taking fluid from the joint. This test helps find the bacteria. You should not give antibiotics before this test, or the results may be wrong. For big joints, doctors use arthroscopic lavage. When the infection is better, start moving the joint. To see if treatment is working, check for pain, swelling, fever, blood tests, and joint fluid.
Doctors say you should:
- Drain the infected joint right away.
- Give antibiotics after you take joint fluid for testing.
- Use arthroscopic lavage for big joints like knees or shoulders.
- Move the joint when the infection is under control to stop stiffness.
The guidelines also say to watch for signs that treatment is not working. These signs are pain, swelling, or fever that do not go away. You should check blood and joint fluid to see if the infection is getting better.
- The guidelines say to use oral antibiotics for 2–4 weeks.
The right time for antibiotics depends on the joint size and how the patient does. Most people need at least two weeks of antibiotics. Some people may need up to four weeks.
Early Diagnosis and Management
You help stop joint damage by acting fast. The guidelines say to find and treat the infection quickly. If you wait too long, the joint can be hurt forever.
A study showed no big difference in CRP levels between early and late surgery. But doctors still say to treat early. Other important things were not studied, so early treatment is still best. Past research shows that early care stops long-term problems and cartilage damage.
- Waiting too long or not treating septic arthritis well can destroy the joint and cause disability.
- It is very important to find the problem fast and start treatment right away.
- Septic arthritis needs quick diagnosis and good treatment to stop bad joint damage and disability.
Remember, every hour matters. Early drainage and antibiotics can save the joint and help people get better faster. The guidelines are clear: act fast, drain the joint, and use the right antibiotics for the right time.
Diagnostic Approach
Clinical Assessment
You look for signs that suggest septic arthritis. Some symptoms make it more likely. If someone has a fever, cannot put weight on the joint, or has high blood test results like ESR or white blood cell count, it helps you decide. The table below shows which signs are most helpful:
| Clinical Indicator | Odds Ratio (OR) | 95% Confidence Interval (CI) | p-value |
|---|---|---|---|
| History of fever | 6.04 | 2.44–14.97 | <0.001 |
| Non-weight-bearing status | 5.23 | 1.38–19.75 | 0.015 |
| Erythrocyte sedimentation rate (ESR) | 3.98 | 1.29–12.30 | 0.017 |
| Serum white blood cell count (WBC) | 2.73 | 1.23–6.03 | 0.013 |
| C-reactive protein | 7.12 | 0.59–85.70 | 0.122 |
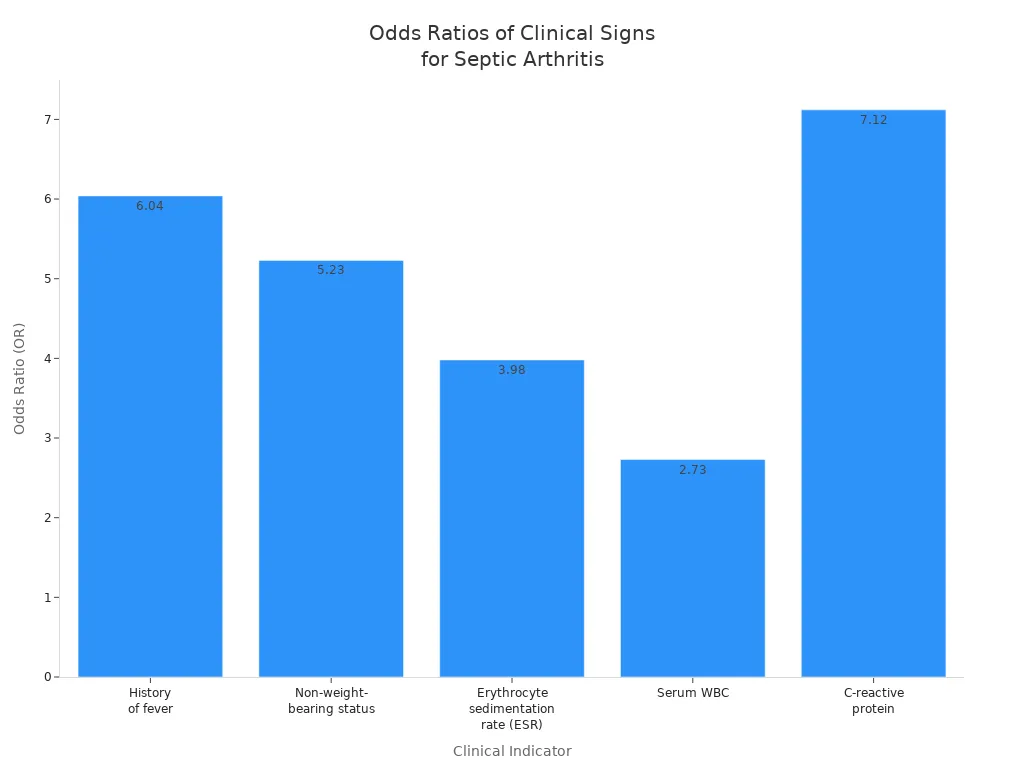
One symptom alone does not prove septic arthritis. You need to look at everything together. Sometimes, just the history and exam do not give you the answer.
Lab and Imaging
Lab tests and imaging help you find out why the joint is swollen. Blood tests like ESR, C-reactive protein, and white blood cell count show if there is inflammation.
Imaging, like X-rays or ultrasound, can show fluid in the joint or rule out other causes. But these tests do not always give a clear answer.
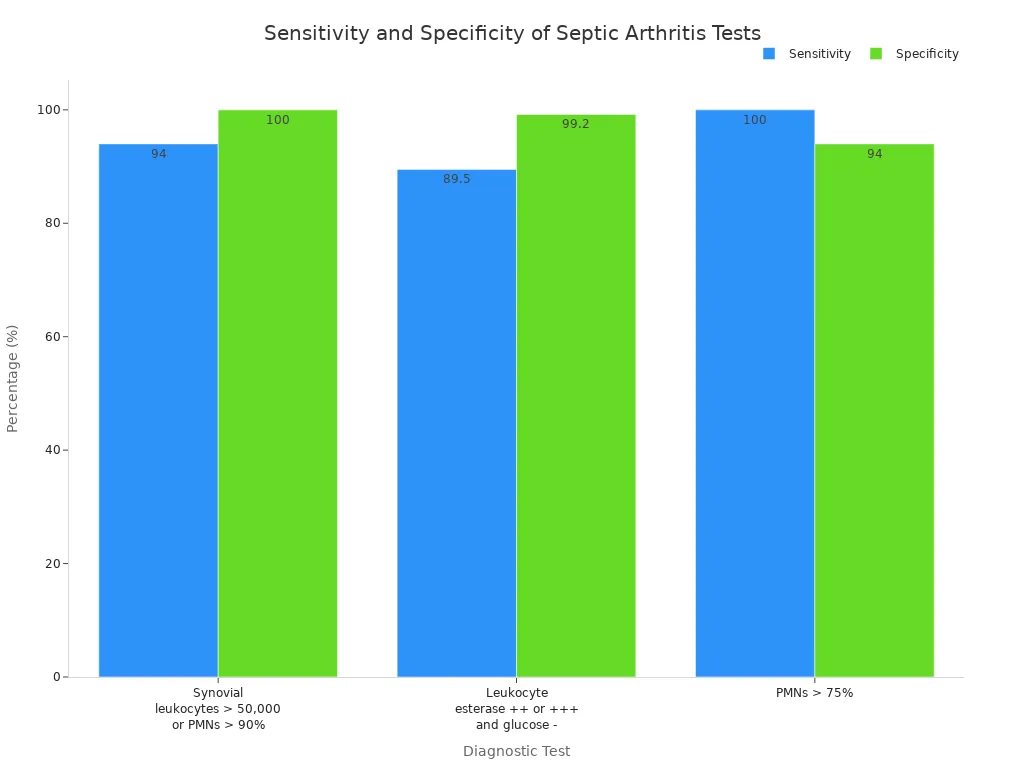
Some lab tests are more accurate than others. For example, if the synovial white blood cell count is over 50,000 or neutrophils are high, infection is very likely.
The table below shows how well some tests work:
| Test | Sensitivity (%) | Specificity (%) | Positive Likelihood Ratio | Negative Likelihood Ratio |
|---|---|---|---|---|
| Synovial leukocytes > 50,000 or PMNs > 90% | 94 | 100 | ||
| Leukocyte esterase ++ or +++ and glucose – | 89.5 | 99.2 | 111.88 | |
| PMNs > 75% | 100 | 94 | 16.67 |
If the synovial white cell count is high and there are no crystals, infection is very likely.
Synovial Fluid Analysis
You need to take fluid from the joint to confirm septic arthritis. This test gives you the best chance to find the cause.
A high white blood cell count in the fluid, especially if neutrophils are over 90%, almost always means infection. Some important things to remember:
- Synovial fluid analysis finds septic arthritis about 61% of the time.
- If calprotectin in the fluid is less than 52 mg/L, infection is not likely.
- A neutrophil count below 15,000 also means infection is not likely.
You should always use the synovial fluid results with your other findings and lab tests. The septic arthritis treatment guidelines say to test joint fluid early to help you decide what to do next.
Microbiological Methods
Sample Collection
You help find out what causes septic arthritis. Collecting good samples is very important. You must take synovial fluid before giving antibiotics.
This step helps you find the bacteria. If surgery is needed, take tissue samples from inside the joint too. Sometimes, tissue samples show bacteria when fluid tests do not.
To get the best results, do these things:
- Take samples right after you think there is an infection.
- Use clean containers to keep the sample safe.
- Put synovial fluid into blood culture bottles. This can help you find more bacteria.
- Send the samples to the lab fast so results are correct.
Using both synovial fluid and tissue samples helps you find the germ that causes the infection.
Always handle samples carefully. Fast and clean work helps you avoid mistakes. This gives you the best chance to help your patient.
Pathogen Identification
You need to find out which germ is causing the infection. Labs use different ways to find the pathogen. Each way works better or worse.
Multiplex PCR finds bacteria in about 63% of cases. Standard culture works in about 26% of cases. mNGS finds the germ in about 11% of cases.
| Method | Success Rate (%) |
|---|---|
| Multiplex PCR | 63 |
| Standard Culture | 26 |
| mNGS | 11 |
Use the best test your hospital has. If the first test does not find the germ, try another test. Knowing the exact germ helps you pick the right antibiotic and helps your patient get better.
Joint Drainage
Indications
You need to know when to drain a joint in septic arthritis. Look for these signs in your patient:
- Sudden joint pain without injury
- Swelling and warmth in the joint
- Fever that comes with joint symptoms
Older adults, people with diabetes, or those who use immune-suppressing medicines have a higher risk. If your patient has had recent joint surgery or has a prosthetic joint, you should be extra careful.
Sometimes, skin infections near the joint can also lead to septic arthritis. You can use blood tests like erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) to help you decide, but these tests do not give a clear answer by themselves.
The most important step is to take fluid from the joint and test it. This test confirms the diagnosis and helps you choose the right treatment.
Always collect synovial fluid before starting antibiotics. This gives you the best chance to find the cause of infection.
Timing and Methods
You should drain the infected joint as soon as possible. Early drainage helps remove bacteria and reduces pressure inside the joint.
This step protects the cartilage and stops further damage. For most patients, you can start with daily needle aspirations. This method works well for simple cases and lets you check the joint each day.
If you cannot get all the fluid out, or if the joint is hard to reach (like the hip), you may need surgery. Surgery is also the best choice if your patient does not get better after three to five days of needle drainage. Sometimes, you cannot dry the joint with a needle. In these cases, surgical drainage is safer and more effective.
- Start with daily needle aspiration for most joints.
- Choose surgery for joints you cannot reach, or if needle drainage does not work after a few days.
- Watch your patient closely. If symptoms do not improve, switch to surgical drainage.
You play a key role in protecting the joint. Fast action and the right drainage method help your patient recover and keep their joint healthy.
Antibiotic Therapy
Empirical Treatment
You should start antibiotics right away if you think it is septic arthritis. Do not wait for lab results if the patient is very sick.
Pick antibiotics based on the germs that usually cause this and the patient’s history. If the Gram stain does not show bacteria, think about the patient’s age and if they are sexually active.
Young adults who are sexually active often get gonococcal arthritis. Older people or those with joint replacements may have other bacteria.
- Your first treatment should cover Staphylococcus aureus, streptococci, and gonococci.
- Use ceftriaxone and vancomycin as your main antibiotics.
- Add rifampin if the patient has an artificial joint or something else implanted.
- Do not put antibiotics straight into the joint. This can hurt the cartilage.
- Most people need 3 to 4 weeks of treatment. If the infection is from gonococci, 2 weeks is usually enough.
Collect joint fluid for testing before you start antibiotics. This helps you find the cause and pick the best medicine.
Targeted Therapy
When the lab tells you which germ is causing the infection, change the antibiotics to match it. This helps treat the infection better and lowers side effects.
If you give antibiotics before taking samples, it can be harder to find the germ. The table below shows how this can change your results:
| Group | Preoperative Culture Yield | Operative Culture Yield | Change in Yield |
|---|---|---|---|
| Preoperative Antibiotics | 68.8% | 57.1% | Decrease |
| No Preoperative Antibiotics | 60.9% | 67.4% | Increase |
Using culture results helps you make better treatment choices. Always change your plan when you get new lab results.
Duration and Route
Start with intravenous antibiotics for the first 1 to 2 weeks. When the patient feels better and the infection is under control, you can switch to oral antibiotics.
This way works well and helps patients leave the hospital sooner. Studies show that early oral therapy helps people get better faster and does not cause more side effects.
- Treat small joints for at least 2 weeks.
- Treat large joints for 4 to 6 weeks.
- Always watch for signs that the infection is coming back, especially if you use a shorter treatment.
You help your patient get better faster by switching to oral antibiotics when it is safe. Always make sure the patient is stable before you make the change.
Post-Procedure Care
Rehabilitation
You help your patient get better after septic arthritis. Starting rehab early is very important. Early physiotherapy helps the joint move again and makes it stronger.
It also lowers pain and helps your patient do normal things. There are different ways to help your patient recover.
The table below lists some of the best methods:
| Rehabilitation Strategy | Outcome Description |
|---|---|
| Early physiotherapy rehabilitation | Helps the joint move, builds strength, lowers pain, and lets your patient do daily things. |
| Conventional physiotherapy | Makes the joint move better, builds strength, and helps your patient do more on their own. |
| Therapeutic approaches (passive movement, CPM, isometric exercises, gait training) | Helps the knee work better and makes life better. |
You can use passive movements or a CPM machine to help the joint move. Isometric exercises and gait training help your patient walk and feel stronger. Tell your patient to start moving the joint when the infection is better. This stops stiffness and keeps muscles strong.
Moving early and doing exercises helps your patient get back to normal faster.
Pain Management
You want your patient to feel less pain while healing. Good pain control helps your patient move and get better. There are many ways to help with pain:
- Give pain medicine like ibuprofen or acetaminophen.
- Suggest rest and keep the joint still for a short time.
- Raise the joint to help with swelling.
- Put a cool pack on the joint.
- Encourage gentle exercise to help healing.
You can also help your patient get better by doing these steps:
- Help your patient move the joint again.
- Support muscle strength with easy exercises.
- Use crutches or canes if needed.
- Keep doing rehab to build muscle, move the joint, and help balance.
You help your patient heal by using pain control and the right exercises. This helps your patient get back to daily life faster and safer.
Monitoring Outcomes
Response Markers
You need to check if your patient is getting better after starting treatment for septic arthritis. You can use both clinical signs and lab tests to track progress. Watch for less pain, less swelling, and lower fever. These changes show that the infection is under control.
Lab tests help you see if the body is fighting the infection. Some markers work better than others. You can use the following table to compare how well each biomarker works:
| Biomarker | Specificity | Sensitivity |
|---|---|---|
| CD64 | 98% | 59% |
| PCT | 98% | 52% |
| CRP | N/A | N/A |
| WBC | N/A | N/A |
| ESR | N/A | N/A |
CD64 and PCT have high specificity. This means if these markers are high, your patient likely still has an infection. Sensitivity is lower, so a normal result does not always mean the infection is gone. You should use these markers with other signs, not alone.
You can also look at how well these tests predict treatment response:
| Metric | Value |
|---|---|
| Sensitivity | 54% |
| Specificity | 95% |
| Positive Likelihood Ratio | 10.97 |
| Negative Likelihood Ratio | 0.49 |
| AUROC | 0.82 |
A high specificity and positive likelihood ratio mean these tests are good at confirming infection. Always check both lab results and how your patient feels.
If pain, swelling, and fever go down and lab markers improve, your patient is likely getting better.
Treatment Failure
You must watch for signs that treatment is not working. If your patient still has pain, swelling, or fever after a few days, you should worry about treatment failure. Sometimes, lab markers like CRP or WBC stay high. This can mean the infection is not under control.
Look for these warning signs:
- No change or worse pain and swelling
- Fever that does not go away
- Lab markers that stay high or go up
- New redness or pus around the joint
If you see these signs, you may need to drain the joint again or change antibiotics. Always talk with your team and act fast to protect the joint.
Early action can prevent long-term joint damage if you spot treatment failure quickly.
Special Scenarios
Children
You must act fast if you think a child has septic arthritis. Waiting too long can hurt the joint forever. Watch for these signs: fever, pain, swelling, and warmth in the joint.
Finding the problem early helps stop joint damage. Start antibiotics right away if you think bacteria are causing it. Drain pus from the joint if needed. Help with pain and begin physical therapy as soon as you can.
Kids get better when you treat them quickly and help them move early.
Post-ACL Surgery
Septic arthritis after ACL surgery does not happen often, but you need to watch for it. The chance of infection is between 0.14% and 1.8%.
You can lower the risk by picking patients carefully, giving antibiotics before surgery, keeping things clean, and soaking the graft in antibiotics.
If an infection starts, clean and flush the knee with a scope first. If that does not work, you might have to take out the hardware or graft. Wait at least three months before putting in a new graft if you remove it.
Being careful before, during, and after surgery keeps the joint and graft safe.
Tuberculous Arthritis
Tuberculous arthritis needs a different plan than regular septic arthritis. You must use special medicines and treat for a longer time.
The table below shows the main differences:
| Treatment Aspect | Tuberculous Arthritis | Septic Arthritis (Standard Protocol) |
|---|---|---|
| Main Treatment | 3 or 4-drug antimicrobial therapy | Antibiotics based on culture results |
| First-line Drugs | Isoniazid, Rifampicin, Pyrazinamide, Ethambutol | Varies based on pathogen |
| Duration of Initial Treatment | 8 weeks of daily treatment followed by 28-36 weeks | Depends on pathogen and response |
| Surgical Intervention Indications | Marked neurological defect, large abscess, instability | Drainage of abscess, debridement |
| Postoperative Care | Prolonged antimicrobial therapy | May require additional antibiotics |
You must finish all your medicine to keep the infection from coming back.
Other Special Cases
Some patients need extra care based on their symptoms and test results. The table below gives a quick guide:
| Treatment Approach | Description |
|---|---|
| Empiric Antibiotic Treatment | Pick antibiotics based on Gram stain or what you think is causing it. Use vancomycin for gram-positive cocci and ceftriaxone for gram-negative cocci. |
| Synovial Fluid Analysis | Always test joint fluid to help choose the right antibiotics. |
| Evacuation of Purulent Material | Take out pus from the joint with a needle or surgery to keep the joint safe. |
You help patients do better when you match treatment to their needs and test results.
You help keep your patient’s joint safe by acting quickly. Draining the joint early and using antibiotics for the right amount of time are very important. Start with IV antibiotics, then switch to oral medicine. This plan works well for adults and kids. Giving oral antibiotics early helps children get better and does not add more risk.
- Use ultrasound to help find the problem and drain the joint.
- Start antibiotics fast using a clinical prediction model.
- Look out for extra risks like diabetes, rheumatoid arthritis, or if the patient had joint surgery.
Always pay close attention, change your plan if needed, and check your patient often. Acting fast helps people with septic arthritis get better.
FAQ
What is the first thing you should do if you suspect septic arthritis?
You should take fluid from the swollen joint right away. This test helps you find the cause. Do not give antibiotics before you collect the sample.
How long do you need to take antibiotics for septic arthritis?
Most people need antibiotics for 2 to 6 weeks. Small joints usually need 2 weeks. Large joints may need up to 6 weeks. Your doctor will decide based on your progress.
Can you walk or move the joint during treatment?
You should rest the joint at first. When the infection improves, start gentle movement. Early movement helps prevent stiffness and keeps muscles strong.
What signs show that treatment is not working?
- Pain or swelling does not get better
- Fever stays high
- Blood tests do not improve
- New redness or pus appears
If you see these signs, tell your doctor right away.




